
Medical device cybersecurity guidelines are a set of regulatory and technical standards designed to protect patient safety by ensuring connected medical devices resist and respond to cyber threats. The U.S. Food and Drug Administration, the EU Medical Device Coordination Group (MDCG), and standards bodies like AAMI have each published frameworks that define exactly what manufacturers and healthcare organisations must do. Cybersecurity threats in healthcare have escalated to threats to life, with ransomware attacks shutting down critical medical systems. That reality makes compliance not just a regulatory checkbox but a direct patient safety obligation.
What are the main regulatory requirements for medical device cybersecurity guidelines?
The FDA's Section 524B of the Federal Food, Drug, and Cosmetic Act sets the baseline for what the agency calls "cyber devices." Manufacturers must submit a security risk management report, a software bill of materials (SBOM), and a postmarket monitoring plan as part of every premarket submission. The FDA recommends modelling these reports on AAMI TIR57 and ANSI/AAMI SW96, two standards that define how to conduct threat modelling, vulnerability assessments, and risk documentation. These are not optional references. They are the benchmarks reviewers use to evaluate submission quality.
FDA Section 524B requires manufacturers to disclose both resolved and unresolved software anomalies, along with component support timelines. That requirement forces manufacturers to think beyond launch day and plan for the full device lifecycle. Regulators want evidence that a device will remain secure years after it ships.
The EU's framework operates under MDR 2017/745, with MDCG 2019-16 providing the cybersecurity-specific guidance. The EU MDCG guidance aligns cybersecurity risk management with broader healthcare resilience planning and includes provisions for financial support to smaller healthcare providers. The EU approach emphasises risk management as an ongoing obligation, not a one-time design activity.
Key documentation obligations under both frameworks include:
- Security Risk Management Plan: A living document covering threat modelling, risk controls, and residual risk acceptance.
- Software Bill of Materials (SBOM): A complete inventory of every software component, including third-party libraries and their support status.
- Vulnerability Assessment Report: Evidence that known vulnerabilities have been identified, evaluated, and either remediated or formally accepted.
- Postmarket Monitoring Plan: A written commitment to surveillance, coordinated vulnerability disclosure, and timely patching.
- Labelling disclosures: Instructions for healthcare facilities on how to configure and maintain the device securely.
| Requirement | FDA (Section 524B) | EU (MDR / MDCG 2019-16) |
|---|---|---|
| Security risk management report | Mandatory, modelled on AAMI TIR57 | Required within QMS framework |
| SBOM | Mandatory | Strongly recommended |
| Postmarket monitoring plan | Mandatory | Required under MDR lifecycle obligations |
| Vulnerability disclosure programme | Mandatory | Required |
| Labelling with security instructions | Mandatory | Required |
How to implement cybersecurity risk management throughout the device lifecycle?
Security risk management must be integrated into the Quality Management System from the earliest design phases, not treated as a retrospective patch. ISO 13485, the international standard for medical device quality management systems, provides the process framework. Cybersecurity controls belong inside that framework, not alongside it as a separate workstream.
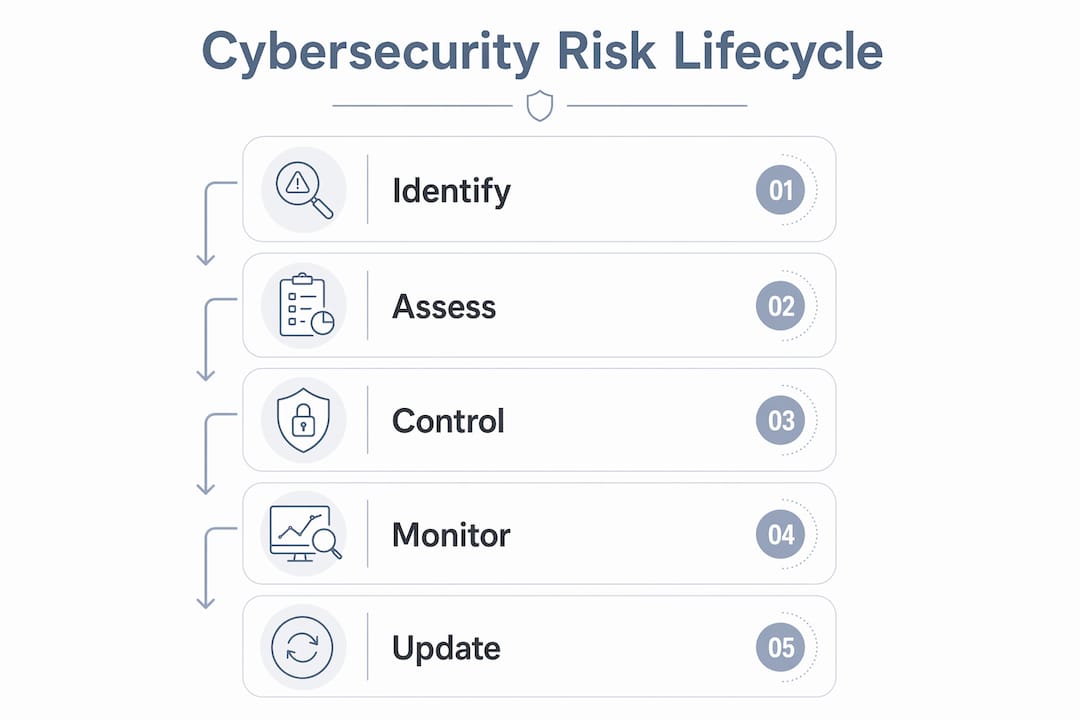
A practical lifecycle approach follows these steps:
- Threat modelling at design: Identify attack surfaces, data flows, and adversarial scenarios before writing a single line of code. Use structured methods such as STRIDE to categorise threats systematically.
- Security requirements definition: Translate threat model outputs into specific, testable security requirements. These feed directly into design specifications and verification protocols.
- Vulnerability assessment during development: Conduct static code analysis, penetration testing, and component scanning before submission. Document findings and remediation actions in the security risk management report.
- SBOM maintenance: Keep the SBOM current throughout development and update it with every software change. An outdated SBOM is a compliance gap and an operational blind spot.
- Coordinated vulnerability disclosure programme: Establish a public-facing process for researchers and healthcare partners to report vulnerabilities. Postmarket surveillance programmes and coordinated disclosure are mandatory under the latest FDA guidance.
- Postmarket monitoring: Monitor threat intelligence feeds, vendor advisories, and national vulnerability databases continuously. Assign ownership so that alerts trigger defined response actions.
- End-of-life planning: Document when software components lose vendor support and plan for device updates or decommissioning before that date arrives.
Pro Tip: Map every cybersecurity control back to a specific clause in ISO 13485 or AAMI TIR57. Reviewers and auditors follow those standards. Showing traceability reduces review cycles and demonstrates that security is embedded in your QMS, not bolted on.
Supplier controls deserve particular attention. Third-party software components introduce vulnerabilities that the device manufacturer inherits. Contracts with software suppliers should require timely notification of security patches and access to updated SBOMs. Many manufacturers overlook this until a critical vulnerability surfaces in a widely used library.

What technical and organisational controls strengthen medical device cybersecurity?
Effective cybersecurity controls combine technical measures like multi-factor authentication and zero-trust architecture with organisational commitment and staff training. Technical controls alone do not produce resilience. The human layer is where most breaches begin.
Technical controls that compliance officers should verify are in place:
- Multi-factor authentication (MFA): Required for all administrative access to networked devices and supporting infrastructure. MFA blocks the majority of credential-based attacks.
- Network segmentation: Medical devices should operate on isolated network segments. Flat networks allow a single compromised endpoint to reach every connected device.
- Zero-trust architecture: Treat every connection as untrusted until verified. Zero-trust removes the assumption that internal network traffic is safe, which is a dangerous assumption in hospital environments.
- Patch management: Define maximum acceptable patch deployment timelines and enforce them. Unpatched devices are the most common entry point for ransomware.
- Encryption: Encrypt data in transit and at rest. This applies to device communications, stored patient data, and backup systems.
- Audit logging: Maintain tamper-evident logs of all access and configuration changes. Logs are the primary evidence source during incident investigations.
Pro Tip: Conduct a cloud security posture review for any medical device that connects to cloud-hosted services. Cloud misconfigurations are a leading cause of data exposure in healthcare environments.
Organisational controls are equally critical. Clinical staff interact with medical devices daily and are the first line of defence against phishing, social engineering, and misuse. Regular security awareness training, clear incident reporting procedures, and defined roles for IT, security, and clinical teams all reduce risk. Cybersecurity is no longer solely an IT issue. It requires frontline clinical engagement to produce real resilience.
What are common challenges and pitfalls in meeting device security standards?
Healthcare organisations and manufacturers consistently encounter the same obstacles when working toward compliance. Recognising these pitfalls early prevents costly rework and regulatory delays.
- Treating cybersecurity as an IT-only problem. Security decisions made without clinical input produce controls that clinicians bypass because they interfere with care delivery. Compliance requires cross-functional ownership from the start.
- Neglecting postmarket vulnerability management. Many manufacturers invest heavily in premarket security and then go quiet after clearance. Vulnerabilities discovered after launch require the same rigour as those found during development.
- Underestimating insider threats and human error. Common employee cybersecurity vulnerabilities account for a significant share of healthcare breaches. Phishing, weak passwords, and misconfigured access permissions are preventable with training and policy enforcement.
- Incomplete security risk management documentation. Submissions that lack traceability between identified threats and implemented controls draw immediate scrutiny. Reviewers expect to see a clear chain from threat model to control to test evidence.
- Failing to update the SBOM after software changes. A static SBOM becomes inaccurate within months of device launch. Regulatory expectations treat SBOM maintenance as a continuous obligation, not a one-time deliverable.
The underlying pattern across all five pitfalls is the same. Organisations treat cybersecurity as a project with a defined end date rather than as a permanent operational discipline. Regulators on both sides of the Atlantic have designed their frameworks specifically to close that gap.
How to maintain and update medical device cybersecurity as guidelines evolve?
Regulatory requirements for protecting medical devices will continue to tighten. The FDA has signalled further guidance updates, and the EU's NIS2 Directive adds another layer of obligation for healthcare operators. Staying current requires a structured maintenance programme, not periodic reviews.
Practical maintenance activities include:
- Continuous threat intelligence monitoring: Subscribe to feeds from the Cybersecurity and Infrastructure Security Agency (CISA), the National Vulnerability Database (NVD), and device-specific vendor advisories.
- Scheduled SBOM reviews: Audit the SBOM quarterly and after every software update. Flag components approaching end-of-support and initiate replacement planning.
- Coordinated vulnerability disclosure updates: Review and test your disclosure process annually. Researchers and partners need a clear, responsive channel.
- Regulatory horizon scanning: Assign a compliance officer to monitor FDA guidance updates, EU regulatory amendments, and AAMI standard revisions. Changes often include transition periods, but those windows close quickly.
- Annual security training refreshes: Update training content to reflect new threat types. Enterprise vulnerability management processes provide a useful framework for structuring ongoing staff education alongside technical controls.
The U.S. healthcare sector experienced 460 ransomware attacks in 2025, making it the most targeted critical infrastructure sector. That figure reflects what happens when postmarket vigilance lapses. Maintenance is not overhead. It is the core of a defensible security programme.
Key takeaways
Effective medical device cybersecurity requires continuous integration of regulatory standards, technical controls, and organisational practices across the full device lifecycle.
| Point | Details |
|---|---|
| Regulatory frameworks are mandatory | FDA Section 524B and EU MDR/MDCG 2019-16 require documented security risk management, SBOM, and postmarket plans. |
| SBOM maintenance is ongoing | Update the software bill of materials after every software change, not just at premarket submission. |
| Cross-functional ownership is required | Cybersecurity decisions must involve IT, clinical, and compliance teams to produce controls that work in practice. |
| Postmarket vigilance prevents breaches | Continuous threat monitoring and coordinated vulnerability disclosure are mandatory under current FDA guidance. |
| Documentation quality determines outcomes | Incomplete or non-traceable security risk management reports are the most common cause of regulatory delays. |
Where regulatory compliance meets clinical reality
The most persistent mistake I see in healthcare cybersecurity is the assumption that regulatory compliance and clinical operations are in tension. They are not. The FDA and EU frameworks are designed to produce devices that are genuinely safer, not just better documented. When compliance officers treat the security risk management report as a filing exercise rather than a working tool, they miss the point entirely.
What actually works is early, repeated engagement between regulatory, IT, and clinical teams. Security requirements that clinicians help define are requirements that clinicians will respect. Controls designed without clinical input get disabled within weeks of deployment because they slow down care. That is not a security culture problem. That is a design problem.
I also think the industry underestimates how much the zero-trust model changes the calculus for medical devices. Perimeter defences made sense when devices were isolated. They do not make sense when an infusion pump connects to a cloud-hosted pharmacy system and a hospital's electronic health record simultaneously. Zero-trust treats every connection as a potential threat, which is exactly the right posture for that environment.
The regulatory landscape will keep moving. The organisations that build cybersecurity into their quality management systems now, rather than retrofitting it before each submission, will handle those changes without crisis. The ones that treat it as a compliance sprint will keep running the same race.
— Nick, Sr. Executive
How AccountNext-Nexus supports medical device cybersecurity compliance
Healthcare organisations navigating the demands of FDA Section 524B and EU MDR cybersecurity requirements need more than policy documents. They need continuous monitoring, expert guidance, and technical controls that work in clinical environments.
AccountNext-Nexus provides 24/7 threat detection and monitoring tailored to healthcare environments, including networked medical devices and the infrastructure that supports them. The team brings direct experience with regulatory documentation requirements, risk management frameworks, and postmarket surveillance programme design. Whether you are preparing a premarket submission or responding to a newly discovered vulnerability, AccountNext-Nexus consolidates the cybersecurity and compliance support you need under one provider. Contact the team to discuss how these services apply to your device portfolio and compliance obligations.
FAQ
What are medical device cybersecurity guidelines?
Medical device cybersecurity guidelines are regulatory and technical standards that require manufacturers and healthcare organisations to protect connected devices from cyber threats throughout their lifecycle. Key frameworks include FDA Section 524B, EU MDR/MDCG 2019-16, AAMI TIR57, and ANSI/AAMI SW96.
What is an SBOM and why does it matter for compliance?
A software bill of materials (SBOM) is a complete inventory of every software component in a medical device, including third-party libraries and their support status. The FDA requires an SBOM in premarket submissions and expects manufacturers to keep it current after device launch.
How does FDA Section 524B affect premarket submissions?
FDA Section 524B requires manufacturers of cyber devices to include a security risk management report, an SBOM, resolved and unresolved anomaly disclosures, and a postmarket monitoring plan in every premarket submission.
What is the biggest compliance mistake healthcare organisations make?
The most common mistake is treating cybersecurity as a premarket activity rather than a continuous lifecycle obligation. Postmarket vulnerability management and SBOM maintenance are mandatory under current FDA guidance and must continue for the life of the device.
How often should security risk management plans be updated?
Security risk management plans should be reviewed and updated whenever a software change occurs, when a new vulnerability is identified, or when regulatory requirements change. Annual reviews at minimum are considered standard practice under current guidelines.